
In 2022, a group of interested physiotherapists and exercise physiologists decided to increase awareness of hypermobility disorders within the physiotherapy profession. Read more about the hypermobility disorder advocacy group and their plans here: https://www.hypermobilityconnect.com/hypermobility-lectures/
Not Just Bendy Hypermobility Services founder, Sharon Hennessey, presented a zoom webinar titled “Hypermobility: its types and its management” to a group of close to 500 physiotherapist and other health professionals.
In-motion magazine (the monthly magazine printed by the Australian Physiotherapy Associate for all of its members) included a 6 page article to try to make physios think about hypermobility when looking at their clients.
The article has been reproduced here in a series of images Switching on the Lightbulb to see Hypermobility Disorders:
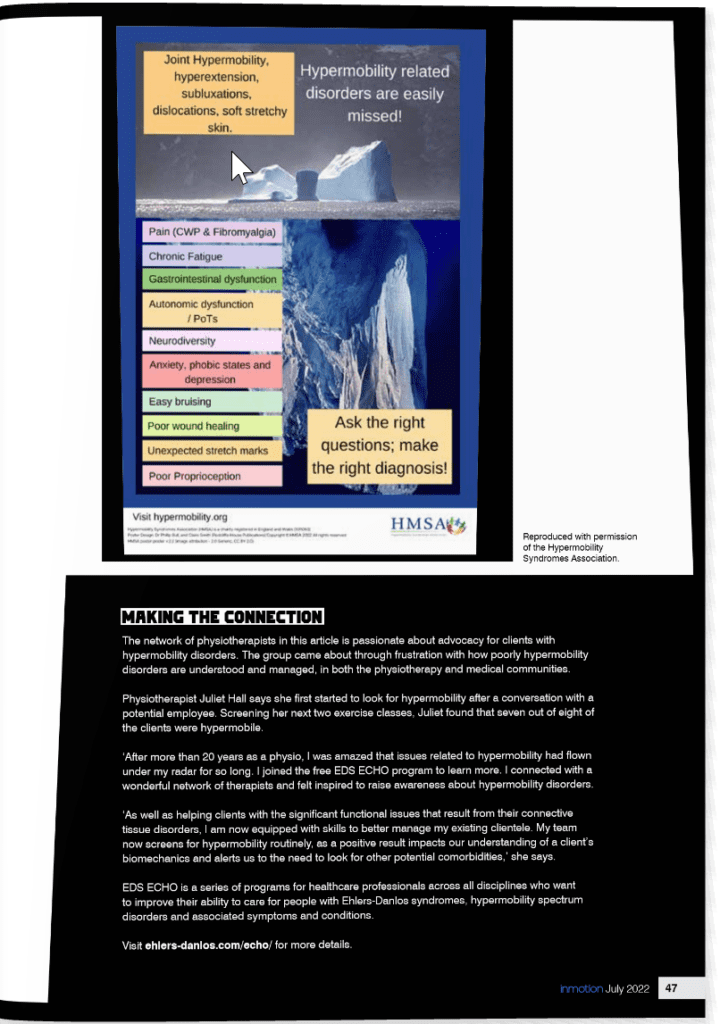
Sharon Hennessey is very passionate about the importance of recognition/diagnosis of hypermobility disorders and here is a selection, from the article, where she explains why she believes this is essential.
“In recently published Masterclass in Hypermobility, internationally renowned physiotherapist, Jane Simmons states, “Early recognition and treatment of hypermobility related disorders is key to effective management.”
Sharon Hennessey, is also adamant, stating, “Just because it is common – does not mean it should be ignored. Obesity is common. Depression is common, but clients are offered appropriate medical care for these issues. Hypermobility should be given the same respect. It isn’t simply chronic pain that is experienced by these clients, there are additionally frequent acute and sub-acute local tissue issues that are still healing, often wrapped up in a package of sensory sensitisation.”
Earlier in her career, Sharon had a 17-year-old client (BB) who was referred for lateral hip pain. On the first appointment, she seemed a little distant and laughed when talking about her pain, saying, “I am just weird.” BB had seen multiple physios throughout her life and was often discharged due to failure to progress. BB was very intelligent, in in her first term of Occupational Therapy, but was struggling with her workload, suffering with fatigue, dizziness and pain flare ups.
On deeper probing Sharon found out that:
- BB was falling weekly due to her ankles giving way or sometimes due to black outs.
- She had fractured both her wrist and fibula in the last 6 months.
- She had failed an adolescent pain clinic and had CRPS in her elbow from a previous injury while at high school.
- She complained of gut pain and had difficulty maintaining her weight.
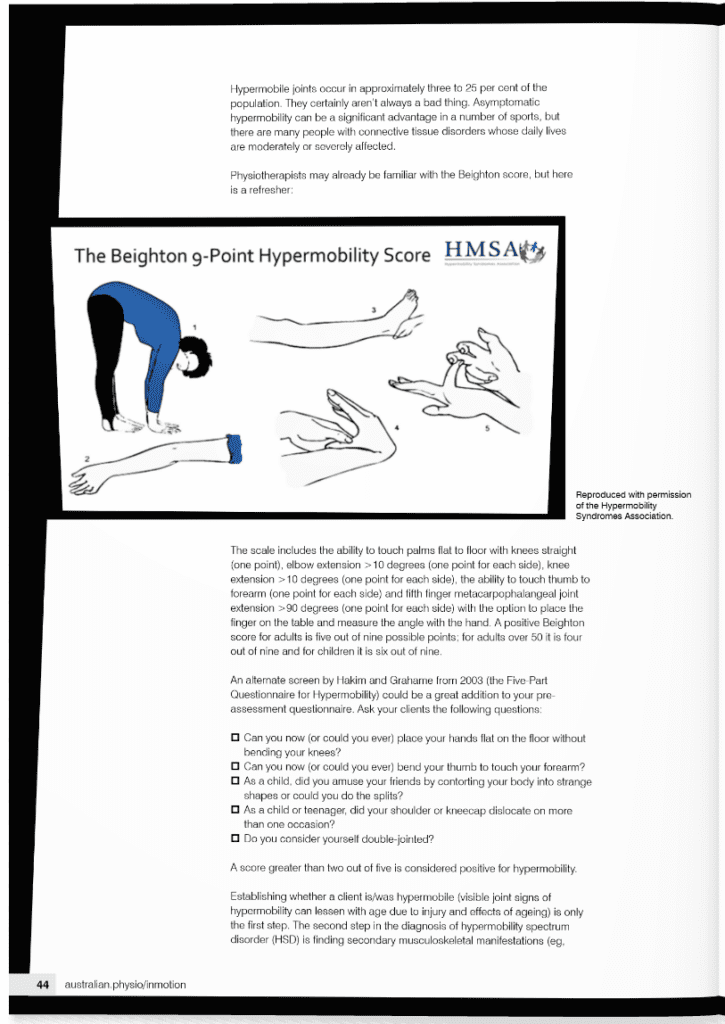
- Beighton score: 9/9
- 5-Part Questionnaire for Hypermobility Score: 3/5
Sharon put together her issues and recognised her Hypermobility Spectrum Disorder.
Despite doing her exercises, eight weeks later, BB did not progress with her control of her one leg balance and she did not report any reduction in pain levels. This is not unusual with clients with hypermobility, so treatment continued, and she made significant gains but over a much longer period than would have been expected with a regular client. Letters were sent to her GP as well as a session with her family to explain HSD. The multidisciplinary team became involved including psychology, dietetics, podiatry, cardiology and genetics (for h-EDS assessment) as well as a weekly clinical Pilates class.
BB’s progress often hit roadblocks including an ankle stabilisation (with CRPS complication), her passing out in the clinic from malnutrition (due to gastroparesis) and insertion of a PEG (for supplemental feeds). But the rewards for working with BB long term have been enormous including see her self-worth build when she got her official H-eds diagnosis, seeing her graduate from university and successfully work full time as an occupational therapist.
The average time between onset of symptoms and diagnosis with a hypermobility disorder is 10 years. 80-90% of hEDS and HSD clients first present with pain. Our group would love the time between onset of symptoms to diagnosis to be shorter. Will you be a part of that change? “
There is still opportunity to attend the remaining 4 lectures planned by the Hypermobility Disorder Advocacy Group. Full details are available here: https://www.hypermobilityconnect.com/hypermobility-lectures/
They are on the following topics and how they related and how they are influenced by hypermobility disorders:
- Pain
- Paediatrics
- Women’s Health
- Fatigue and Dysautonomia/POTS
References:
- The Ehlers Danlos Society https://www.ehlers-danlos.com/
- Diagnostic Criteria for Hypermobile Ehlers-Danlos Syndrome (hEDS) https://ehlers-danlos.com/wp-content/uploads/hEDS-Dx-Criteria-checklist-1.pdf
- Tinkle B, Castori M, Berglund B, et al. Hypermobile Ehlers-Danlos syndrome (a.k.a. Ehlers-Danlos syndrome Type III and Ehlers-Danlos syndrome hypermobility type): clinical description and natural history. Am J Med Genet C Semin Med Genet. 2017; 175:48–69.
- Castori M, Tinkle B, Levy H, Grahame R, Malfait F, Hakim A. A framework for the classification of joint hypermobility and related conditions. Am J Med Genet C Semin Med Genet. 2017; 175:148–157.
- Kumar,B. Lenert, P. Joint Hypermobility Syndrome: Recognizing a Commonly Overlooked Cause of Chronic Pain, American Journal of Medicine. VOLUME 130, Issue 6 https://doi.org/10.1016/j.amjmed.2017.02.013
- Malfait F, Francomano C, Byers P, Belmont J, Berglund B, Black J, Bloom L, Bowen JM, Brady AF, Burrows NP, Castori M, Cohen H, Colombi M, Demirdas S, De Backer J, De Paepe A, FournelGigleux S, Frank M, Ghali N, Giunta C, Grahame R, Hakim A, Jeunemaitre X, Johnson D, Juul-Kristensen B, Kapferer-Seebacher I, Kazkaz H, Kosho T, Lavallee ME, Levy H, Mendoza-Londono R, Pepin M, Pope FM, Reinstein E, Robert L, Rohrbach M, Sanders L, Sobey GJ, Van Damme T, Vandersteen A, van Mourik C, Voermans N, Wheeldon N, Zschocke J, Tinkle B (2017) The 2017 international classification of the Ehlers-Danlos syndromes. Am J Med Genet C: Semin Med Genet 175(1):8–26. https://doi.org/ 10.1002/ajmg.c.31552
- Jane V. Simmonds, Advances in assessment of hypermobility-related disorders, American Journal of Medical Genetics Seminars in Medical Genetics, Part C (IF3.908), Pub Date: 2021-11-06, DOI: 10.1002/ajmg.c.31943
- J.V. Simmonds, Masterclass: Hypermobility and hypermobility related disorders, Musculoskeletal Science and Practice, Volume 57, 2022, ISSN 2468-7812, https://doi.org/10.1016/j.msksp.2021.1024