
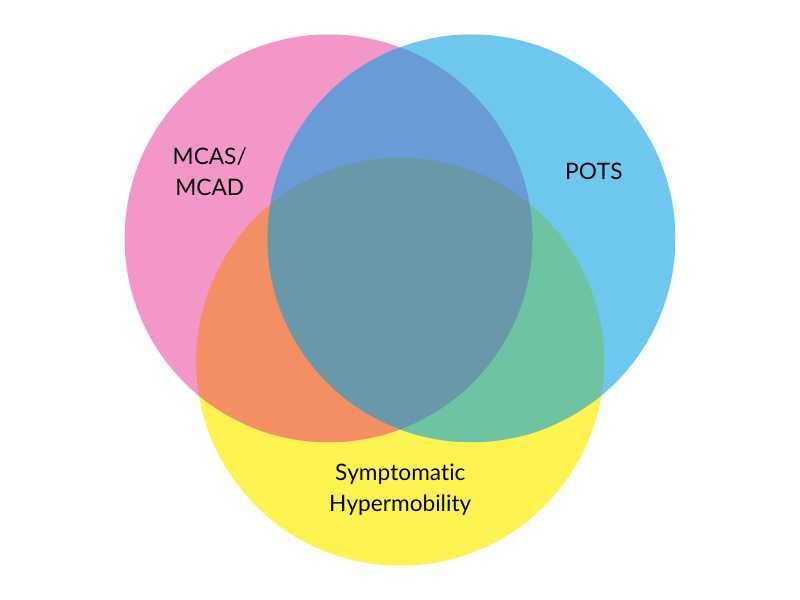
There is a significant overlap in the conditions and the symptoms of MCAS, POTS and symptomatic hypermobility. Learn more in this informative blog.
From an early age, I never really coped with band aids and would always end up with a rash. By mid 20s, I knew using strapping tape on myself was not a solution due to the harsh skin reactions (a problem, as I was burning out as a physio working 55 hours a week and I needed external joint support via tape to get through). Gardening also started to become problematic, as my skin would have a similar reaction if Australian Native Plants touched me.
I knew I was odd and reacted in strange ways to medications – lots of side effects for some and no effects for others. I started to learn to only try new medications on a weekend and at half the recommended dose to give my body time to recover. I, of course, battled my hypermobility and POTS without a lot of understanding until my children were born in my early 30s. Then, I began to realise a lot of my management strategies (rest, electrolytes, pacing, salt, strength exercises) finally made sense.
But Mast Cell Activation Disorder (MCAS) caught up with me when I was in my early 40s and suffered with idiopathic urticaria (unexplained hives all over my body). Everyone told me I was stressed or allergic to something, but I seemed to be allergic to the world! Anything I touched or anywhere I had clothing – socks, shoes, underwear, and pants left me with raised welts for days. I now know this is called dermatographia. Dermatographia, also known as skin writing, is a condition in which the skin becomes raised and inflamed when it is stroked or scratched lightly. This condition is believed to be caused by an over-reaction of the mast cells in the skin.
My first bout of urticaria lasted about 3 months and settled with antihistamines. Eventually, I forgot all about it as it was just another “one of those things.” However, the second bout started 9 months later and lasted for nearly 18 months. Imagine having 400 mozzie (mosquito) bites all over your body, extremely itchy all the time. If I scratched them, I ended up bruised. It wasn’t until I took a truck load of medication and injections (see the medications list below as I had them all) AND took mast cell stabilisers, that I am proud to say no hives for nearly two years! This also helped my gut to function better which was a major improvement of my quality of life.
Now, I am still allergic to tape and plants – but at least I know what to do! It is quite possible that MCAS has also been behind many of my other issues such as fatigue, stress, and pain but this is hard to know, as I have been managing my symptoms conservatively my whole life.
Also, before I start explaining MCAS, it is important to note that Postural Orthostatic Tachycardia syndrome (POTS), hypermobile-Ehlers Danlos syndrome and MCAS are frequently connected conditions, as often clients have all three conditions with similar symptoms therefore difficult to distinguish the underlying cause.
MCAS is very hard to explain. And forgive me if I do not make it completely clear. Even as an experienced scientist it has taken a long time for me to have a rudimentary understanding of it all.
Please understand that this information is intended for educational purposes only and is not intended as medical advice. Everyone is encouraged to obtain independent medical advice from their own medical team about their management.
Mast cells are a type of specialized white blood cells that play a vital role in the body’s immune system. They are found in large numbers in the skin, lungs, nerves, vessels, gut, and other organs. Inside the mast cells are hundreds of different mediators which are usually released in a controlled way when the body needs them. Some of these mediators are important in controlling inflammation, stimulating healing, and protecting the body from infection. They are also involved in the production of histamine, which is a key factor in the body’s allergic response, substances that can cause inflammation, allergic reactions, and other responses in the body. These substances can also be involved in the development of autoimmune diseases, allergies, and even certain cancers.
Mast cells are also involved in the production of various hormones, including serotonin and cortisol. Serotonin is a neurotransmitter that is involved in mood regulation, while cortisol is a hormone that helps the body to regulate stress levels. Mast cells may also be involved in the regulation of blood pressure and the production of certain immune cells. When mast cells are over-activated, it can lead to an exaggerated response in the body and a wide range of symptoms, and through this link to hormones they can affect the heart rate/blood pressure and a cascade of other effect of the sympathetic nervous system including POTS (Postural Orthostatic Tachycardia Syndrome).


Mast cells can also play a role in tissue repair, as they can produce growth factors that can help to promote the healing of damaged tissue. Mast cells can be involved in the repair of blood vessels, and they can also play a role in wound healing. Finally, mast cells can be involved in the production of enzymes that can help to regulate the body’s metabolism.
Mast cells can be activated to release mediators by a variety of triggers, including allergens, infections, and certain medications. When activated, mast cells can lead to symptoms such as skin rashes, itching, hives, runny nose, wheezing, and more. In some cases, over-activation of mast cells can lead to mast cell activation diseases/syndrome, which can cause a variety of symptoms.
Someone may suspect they have mast cell activation diseases (MCAS) if they experience a combination of any of the common symptoms (see infographic below). It is thought that between 17-20% (Afrin, 2023) of the world’s population has some sort of Mast Cell Activation problem, as it is thought to underlie asthma, dementia, irritable bowel syndrome, Hypermobile-Ehlers Danlos Syndrome, fibromyalgia, skin rashes, chronic fatigue syndrome, long covid as well as many other common conditions. Unfortunately, the acceptance of MCAS in the medical community is still in its infancy and no education is offered for doctors in their training courses.
A mutation in the Kit gene can lead to the inappropriate production and release of subsets of mast cell mediators. These mediators release into the blood stream and activate a series of cascades that present as inflammation, allergy and in some cases abnormalities of growth.
Symptoms in MCAS may include skin rash or flushing, itching or hives, runny nose or congestion, abdominal cramping or vomiting, diarrhea or constipation, dizziness or fainting, shortness of breath or wheezing, facial swelling, joint pain or swelling, headaches, palpitations or irregular heart rate, excessive fatigue, anxiety or panic attacks, cognitive impairment or memory loss, weight loss or gain, night sweats, fever, hair loss, and unexplained bruising or bleeding.

If you experience any of these symptoms, it is important to speak with a healthcare professional to discuss further testing and treatment options.
Due to the lack of very clear blood tests to identify MCAS, it remains a condition that is poorly understood or accepted by a lot of the medical profession.
Diagnosis of MCAS remains difficult and is often a clinical diagnosis based on symptoms which depends a great deal on who is conducting the assessment. Definitive diagnosis can be obtained through microscopic analysis of gastrointestinal tissue taken during an endoscopy. If you have had an endoscopy in the past, it is worth checking as some collected cells are stored for 5-10 years, therefore testing can be completed on cells that were collected years before. Cells collected during endoscopy can be tested with the CD117 stain to look for excessive mast cells. This can be organised by a medical practitioner.
Other tests are becoming available in Australia now. The problem with blood testing to this point is that it has not been collected, stored, and analysed in an environment that has kept the mediators from breaking down prior to the test being completed ie they need to be collected and transported cold. Elevated heparin can be demonstrated in approx 80% of MCAS clients – but it has a half-life of 1 minute unless refrigerated immediately! This means that the heparin will break down in the sample if left at room temperature for more than one minute. This has made the collection and analysis of heparin in Australian very tricky.
The most effective treatment for mast cell activation syndrome (MCAS) is to manage the underlying cause or environmental irritant. This takes some detective work to figure out if there are any environmental stressors/irritants.

Keeping a diary to track symptoms, foods consumed and products used, can be useful in ascertaining your environmental irritants.
Once a potential allergen has been identified, trying to decrease the exposure to this is essential. Consulting a dietician to trial a low FODMAP or low histamine diet is essential if you are concerned about food reactions. This website can be helpful to find foods that adhere to certain allergies and diet types https://www.whatthebleepcanieat.com. But it highly recommended that you consult a qualified and experienced dietician before you start on any dietary restrictions.
Medications can be used to treat mast cell activation syndrome (MCAS). Antihistamines can help reduce symptoms, but other medications may be helpful.
Over the counter anti-histamines such as Telfast, Clarytine and Zyrtec can be trialled with the assistance of your pharmacist/GP and each works slightly differently so Dr. Afrin ( a medical specialist with an interest in this field) suggests you try each one at a time for two weeks and note which one has the best effect. With medical assistance often a dosage of twice per day can be trialled. These are the first line as such and are the H1 blockers.
Once the best H1 blocker for you has been found, then Dr. Afrin suggested, to stay on the H1 blocker and try the H2 blockers (eg Famodine/nizatidine etc) one at a time and see what works best for you.
A third line of management, “Mast cell stabilizers” can help to prevent mast cell over-activation, while leukotriene receptor antagonists (eg singular/montelukas) can help reduce inflammation caused by leukotrienes. Compounded medication including Ketotifen or sodium cromoglycate can also be helpful for some people. It is important to speak with a healthcare professional to determine the best medication for your individual needs.
The final line of defence is a monoclonal antibody injection knows as omalizumab (or Zolair) but these are only covered by medicare for severe cases of hives and asthma. It is essential to discuss any of these managements with you GP or specialist and some article references are included at the end if you need to provide educational material to your health professionals.
Depending on the individual, management also involves lifestyle modifications, dietary change (avoiding processed food and low histamine diet), improving sleep, psychological support, movement/exercise, and a sense of belonging (support groups and family/friend support).
Other treatments may include supportive therapies such as physiotherapy, acupuncture, and psychotherapy.
Physiotherapy can be an effective treatment for mast cell activation syndrome (MCAS). Physiotherapy can help to reduce inflammation, improve range of motion, and manage pain. When combined with other treatments, such as medications and lifestyle modifications, physiotherapy can help to improve overall wellbeing and quality of life. Physiotherapy can also help to maintain and improve muscle strength, flexibility, balance, coordination, and endurance. Finally, physiotherapy can help to reduce fatigue and stress, which can help to manage MCAS symptoms.
It is important to note that everyone’s treatment plan will be unique, depending on their specific needs. It is important to consult with a healthcare professional to determine the best treatment plan for your own needs. Additionally, it is important to stay informed about the latest research and treatments for MCAS to ensure you are receiving the best possible care.
This over-activation leads to a wide range of symptoms, including dizziness, fatigue, palpitations, headaches, and more. Hypermobile Ehlers-Danlos Syndrome is also related to mast cell activation diseases because those with the condition often experience an increase in mast cell activity, which can lead to a variety of symptoms. Living with these conditions can be managed with lifestyle modifications, medications, and other treatments by health professionals interested in these areas.
References:
Afrin LB, Ackerley MB, Bluestein LS, Brewer JH, Brook JB, Buchanan AD, Cuni JR, Davey WP, Dempsey TT, Dorff SR, Dubravec MS, Guggenheim AG, Hindman KJ, Hoffman B, Kaufman DL, Kratzer SJ, Lee TM, Marantz MS, Maxwell AJ, McCann KK, McKee DL, Menk Otto L, Pace LA, Perkins DD, Radovsky L, Raleigh MS, Rapaport SA, Reinhold EJ, Renneker ML, Robinson WA, Roland AM, Rosenbloom ES, Rowe PC, Ruhoy IS, Saperstein DS, Schlosser DA, Schofield JR, Settle JE, Weinstock LB, Wengenroth M, Westaway M, Xi SC, Molderings GJ. Diagnosis of mast cell activation syndrome: a global “consensus-2“. Diagnosis (Berl). 2020 Apr 22;8(2):137-152. doi: 10.1515/dx-2020-0005. PMID: 32324159.
Afrin, L. Presentations at the Mast Cell Activation Disease Conference: Current Concepts. Brisbane, Australia (March, 2023)
Kohn A, Chang C. The Relationship Between Hypermobile Ehlers-Danlos Syndrome (hEDS), Postural Orthostatic Tachycardia Syndrome (POTS), and Mast Cell Activation Syndrome (MCAS). Clin Rev Allergy Immunol. 2020 Jun;58(3):273-297. doi: 10.1007/s12016-019-08755-8. PMID: 31267471.
Seneviratne, SL, Maitland, A, Afrin, L. 2017. Mast cell disorders in Ehlers–Danlos syndrome. Am J Med Genet Part C Semin Med Genet 175C: 226– 236.
Weinstock LB, Pace LA, Rezaie A, Afrin LB, Molderings GJ. Mast Cell Activation Syndrome: A Primer for the Gastroenterologist. Dig Dis Sci. 2021 Apr;66(4):965-982. doi: 10.1007/s10620-020-06264-9. Epub 2020 Apr 23. PMID: 32328892.